- Visibility 34 Views
- Downloads 3 Downloads
- DOI 10.18231/j.achr.2024.035
-
CrossMark

A rare case report of hurthle cell adenoma mimicking malignancy
Introduction
Thyroid lesions are the most common endocrine diseases, with nodular architecture and follicular pattern of growth often pose difficulties in accurate diagnosis during the assessment of cytologic and histologic specimens.[1] Majority of Thyroid tumours originates from follicular epithelial cells.
Hurthle cell adenomas are rare, benign tumours of the thyroid, accounting for less than 5%. Size more than 4cms rare.[2]
Hurthle cell adenomas are noninvasive, encapsulated tumors which are surrounded by a thin capsule and characterized by cells with abundant granular, eosinophilic cytoplasm with prominent central nucleoli.
These tumors are remain interesting diagnostic phenomena with acknowledged preoperative and intraoperative adversities in discriminating adenomas from carcinomas.
Hurthle cell tumors often challenging to diagnose due to the ubiquity of Hurthle cells ranging from non-neoplastic conditions to aggressive malignancies. Galectin-3 is a human lectin linked to malignant transformation in different organs including thyroid gland. [3]
Aim of Study
To project the importance of histopathological examination in distinguishing between adenoma and carcinoma.
Case Report
History
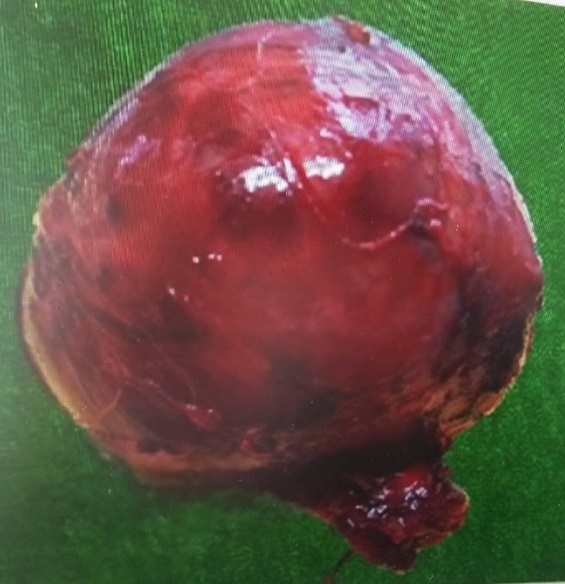
A 72-year-old woman presented with midline diffuse Thyroid swelling in neck since one year, as shown in figure 1. She had no symptoms of weight loss, pain and pressure, hoarseness or fatigue. Her neck swelling was insidious in onset, gradually progressive, initially a size of 2x1 cms and progressed to size of 10x8cms. Physical examination of neck showed a solitary swelling of size 10x8cms present in front of neck more towards right side and moved with deglutition.
Physical examination of neck
A solitary swelling of size 12x8 cms present in front of neck more towards right side and moved with deglutition.
Investigations
Routine Laboratory indices were within normal limits.
Ultrasound of neck
Showed thick walled heteroeic lesion occupying whole of right lobe with a TI-RADS score - Four suggesting Suspicious for malignancy.
FNAC of thyroid swelling
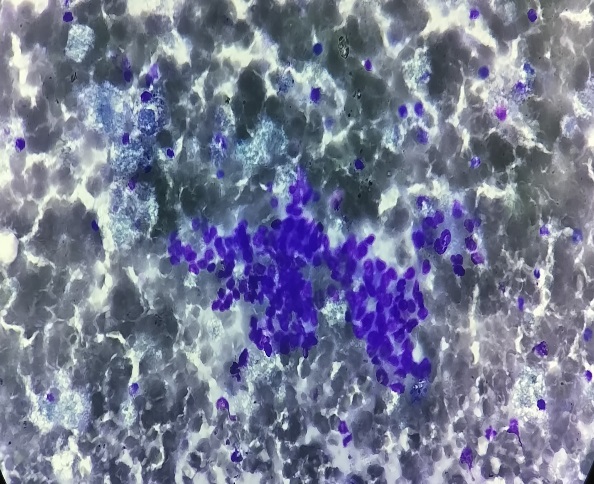
Showed high cellularity comprised of large polygonal cells with nuclear pleomorphism, prominent nucleoli and was reported as SUSPICIOUS FOR MALIGNANCY (The Bethesda System of Reporting Thyroid Cytopathology-V) as in [Figure 2].
Histopathology study
Total thyroidectomy was done, specimen was sent for histopathological study.
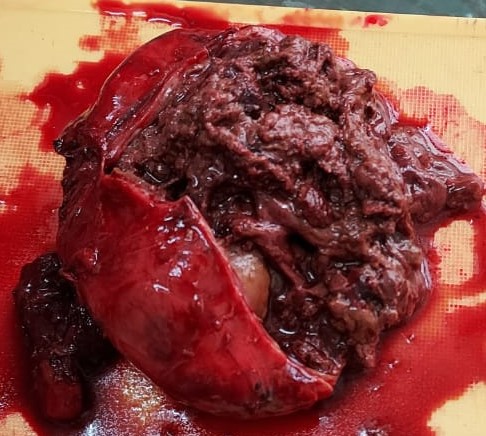
Grossly the mass is as shown in [Figure 3], [Figure 4].
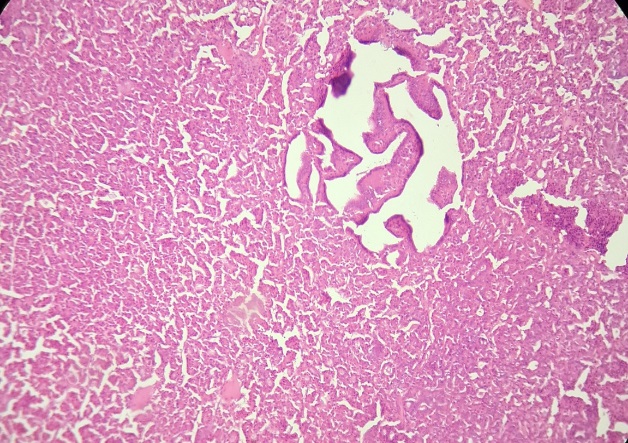
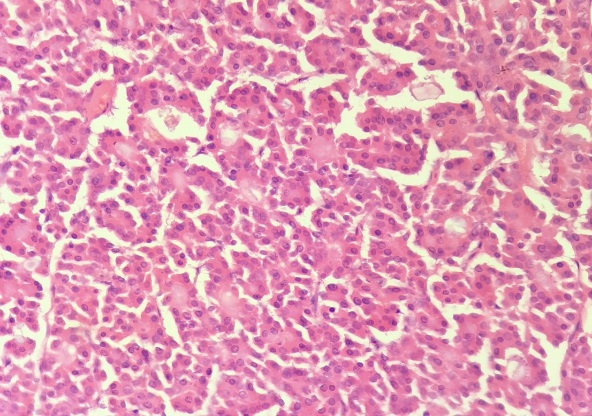
Microscopy revealed a well encapsulated tumor showing oncocytic cells with abundant granular and eosinophilic cytoplasm arranged in micro and macrofollicular pattern, at places papillary pattern. Peripheral thyroid tissue showed features of Nodular Goitre. No evidence of vascular/ capsular invasion was seen in around 60 sections after extensive grossing.
A diagnosis of Hurthle cell/ Oncocytic adenoma in Nodular Goitre was rendered on histopathology as shown in [Figure 5], [Figure 6].
Immunohistochemistry (IHC) study
The tumor was negative for IHC marker Galectin [Figure 7], ruling out Papillary carcinoma of thyroid. However IHC for Ki 67 showed a moderate mitotic activity of 24-26%.
Final diagnosis: Hurthle cell/ Oncocytic adenoma in Nodular Goitre.


Discussion
When compared with classic PTC, DSV has unique clinical features, including a higher prevalence of underlying Hashimoto’s thyroiditis, higher female-to-male ratio, and younger age [4], but in our study, patient is elderly female.
Our case presented with only palpable huge neck mass. As size more than 4cms rare,[2] as similarly in our case, the swelling was 10x8cms, hence our rare entity . Usually thyroid nodules present along with palpable neck mass, anterior neck pain, globus sensation, dysphagia, dyspnea, and dysphonia/ hoarseness.[5]
Till date as similar to our case, poorly differentiated thyroid carcinoma remains a challenge due to its aggressive disease course. [6]
Detection rate of thyroid nodules varies widely in population from 4% to 67%, by physical examination around 4-7%, with a higher detection rate of 30-67% by ultrasound.[7], [8], [9] but in our case patient noticed huge increased in swelling size and came to hospital.
Once the results of a thyroid FNAC are available, the risk of thyroid cancer can be estimated and can guide the next steps in management in patients with benign or malignant results,[10], [11] similarly as in our study FNAC report was suspicious for malignancy (the Bethesda system of reporting thyroid cytopathology-v) guided for further Histopahology and IHC studies.
Hürthle cell adenoma is a rare variant of benign lesion of thyroid gland, however aggressive nature and potential controversies about its malignant nature still remains.
Hürthle cell tumour though rare, yet they are often challenging to diagnose accurately with FNAC, with significant interobserver variability, largely due to the ubiquity of Hürthle cells ranging from nonneoplastic conditions to aggressive malignancies,[12] as in our study FNAC reported as suspicious for malignancy.
Hürthle cell tumors have been associated with various of benign thyroid disorders, including Hashimoto's thyroiditis, hyperthyroidism, nodular goitre, and thyroid neoplasms, where they are thought to be oncocytic metaplasia,[13] as in our study the FNAC report suspicious of malignancy, might be due to potentials of oncocytic metaplasia.
Pre-operative diagnosis is difficult, fine needle aspiration cytology may show Hürthle cell lesions, but final diagnosis is confirmed by histopathology for capsular and vascular invasion,[14] as similarly in our case, FNAC features of suspicious for malignancy and final diagnosis confirmed by histopathology and IHC negative for Galectin-3 study, as retaining importance of histopathology and IHC study as goldstandard investigations for correct diagnosis.
As of the most recent WHO classification, thyroid tumours are a form of tumour that arises from thyroid follicles,[15] as similar in our case, tumour arised from thyroid origin.
As similar studies,[16], [17] ultrasound preoperative diagnosis is difficult. Hürthle cell cancer (HCC) appears as hypoechoic to hyperechoic lesions on ultrasonography, but in our study, thyroid swelling appeared as heteroecoic lesion on ultrasonography.
Similar to in our study, majority of Thyroid neoplams the intraoperative frozen section and FNAC cannot reliably differentiate cancer from adenoma.[18]
Hurthle cell tumors are distinct, not only because of the enduring debate about the true nature, but also because HCC are particularly aggressive, thereby emphasizing the need to differentiate Hurthle cell adenomas from carcinomas.
Hürthle cell carcinoma has a more aggressive clinical course than any other differentiated thyroid carcinoma, with particular drawbacks such as a greater rate of regional lymph node metastases, recurrences, and cause-specific fatality, [19] hence FNAC report was suspicious, hence further proceeded to Histopathology and IHC study.
The differential diagnosis include Hashimoto’s thyroiditis, Nodular goitre, Medullary carcinoma with oncocytic variant and Papillary thyroid carcinoma with oncocytic variant, warthin-like variant and tall cell variant.
The ongoing elucidation of a malignant HCC depends on capsular and/or vascular invasion, and the presence of metastasis. This cannot be determined by cytologic evaluation and relies on histological examination of a resected specimen.
In our case, although being a benign tumor on histopathology and IHC, showed features of malignancy on imaging, cytology and on frozen section.
In addition, Gholami et al.[20] pointed out the FNAC was performed for all the nodules and 39 (70.9%) were benign and 16 (29.1%) were malignant or suspicious for malignancy, were referred for surgery, similarly in our case, for suspicious for malignancy as per FNAC report, total Thyroidectomy was done for further evaluation and diagnosis.
Conclusion
Immunohistochemistry is the most commonly used method to complement morphologic assessment.
Histopathology remains the cornerstone for the diagnosis of thyroid oncocytic lesions and also in distinguishing between adenoma and carcinoma.
Source of Funding
None.
Conflict of Interest
None.
References
- S Et Fischer. Application of immunohistochemistry to thyroid neoplasms. Arch Pathol Lab Med 2008. [Google Scholar]
- RK Singh, A Goyal, P Elhence, A Kumar. Bilateral Hurthle cell adenoma of thyroid: a rare case report. Ijorl.com. cited 2017. [Google Scholar]
- HA Aiad, MA Kandil, NY Asaad, AM El-Kased, SF El-Goday. Galectin-3 immunostaining in cytological and histopathological diagnosis of thyroid lesions. J Egypt Natl Canc Inst 2008. [Google Scholar]
- SM Chow, JKC Chan, SCK Law, DLC Tang, CM Ho, WY Cheung. Diffuse sclerosing variant of papillary thyroid carcinoma- clinical features and outcome. Eur J Surg Oncol 2003. [Google Scholar]
- Jr Et Sørensen, L Hegedüs, S Kruse-Andersen, S Kruse-Andersen, SJ Bonnema. The impact of goitre and its treatment on the trachea, airflow, oesophagus and swallowing function. A systematic review. Best Pract Res Clin Endocrinol Metab 2014. [Google Scholar]
- A Agarwal, G Nelson, K Niraj, K Narendra, M Prabhaker, G Sushil. Poorly differentiated thyroid cancer: Clinical, pathological, mutational, and outcome analysis. Indian J Pathol Microbiol 2024. [Google Scholar] [Crossref]
- S Guth, U Theune, J Aberle, A Galach, CM Bamberger. Very high prevalence of thyroid nodules detected by high frequency (13 MHz) ultrasound examination. Eur J Clin Invest 2009. [Google Scholar]
- C Reiners, K Wegscheider, H Schicha, P Theissen, R Vaupel, R Wrbitzky. Prevalence of thyroid disorders in the working population of Germany: ultrasonography screening in 96,278 unselected employees. Thyroid 2004. [Google Scholar]
- RP Tufano, SI Noureldine, P Angelos. Incidental thyroid nodules and thyroid cancer: considerations before determining management. JAMA Otolaryngol Head Neck Surg 2015. [Google Scholar]
- BR Haugen, EK Alexander, KC Bible, GM Doherty, SJ Mandel, YE Nikiforov. American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2015. [Google Scholar]
- N Singh Ospina, JP Brito, S Maraka, AEE Ycaza, R Rodriguez-Gutierrez, MR Gionfriddo. Diagnostic accuracy of ultrasound-guided fine needle aspiration biopsy for thyroid malignancy: systematic review and meta-analysis. Endocrine 2016. [Google Scholar]
- KS Wong, TE Angell, JA Barletta, JF Krane. Hürthle cell lesions of the thyroid: Progress made and challenges remaining. Cancer Cytopathol 2021. [Google Scholar]
- RK Singh, A Goyal, P Elhence, A Kumar. Bilateral Hurthle cell adenoma of thyroid: a rare case report. Int J Otorhinolaryngol Head Neck Surg 2017. [Google Scholar]
- RM Tambat. Hürthle Cell Adenoma in a Hashimoto’s Thyroiditis Patient: A Rare Case Report. Clin Case Rep 2022. [Google Scholar] [Crossref]
- RV Lloyd, RY Osamura, G Klöppel, J Rosai. . WHO Classification of Tumours of Endocrine Organs 2017. [Google Scholar]
- NO Santana, RMC Freitas, VN Marcos, MC Chammas, RYA Camargo, CK Schmerling. Diagnostic performance of thyroid ultrasound in Hürthle cell carcinomas. Arch Endocrinol Metab 2019. [Google Scholar]
- ZV Maizlin, SM Wiseman, P Vora, JM Kirby, AC Mason, D Filipenko. Hürthle cell neoplasms of the thyroid: sonographic appearance and histologic characteristics. J Ultrasound Med 2008. [Google Scholar]
- H Chen, TL Nicol, R Udelsman. Follicular lesions of the thyroid. Does frozen section evaluation alter operative management?. Ann Surg 1995. [Google Scholar]
- BR Haugen, AM Sawka, EK Alexander, KC Bible, P Caturegli, GM Doherty. American Thyroid Association Guidelines on the Management of Thyroid Nodules and Differentiated Thyroid Cancer Task Force Review and Recommendation on the Proposed Renaming of Encapsulated Follicular Variant Papillary Thyroid Carcinoma Without Invasion to Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features. Thyroid 2017. [Google Scholar]
- M Gholami, L Aghaghazvini, M Gholampour, J Kargar. Evaluation of the diagnostic value of Ultrasound Elastography in TIRADS 4 categories of Thyroid nodules”. J Adv Pharm Edu Res 2021. [Google Scholar]